
What Is SIBO?
Small Intestinal Bacterial Overgrowth (SIBO) occurs when excessive bacteria, often of the wrong kind, colonise the small intestine. While bacteria naturally exist throughout the digestive tract, the small intestine typically contains fewer bacteria than the large intestine. When this balance is disrupted, digestive function can be significantly impaired.
Small Intestinal Bacterial Overgrowth
In this comprehensive article, we’ll explore the prevalence and symptoms, causes and tests of SIBO. For comprehensive information about SIBO treatment and management, including SIBO diet and supplementation, click here: SIBO Treatment

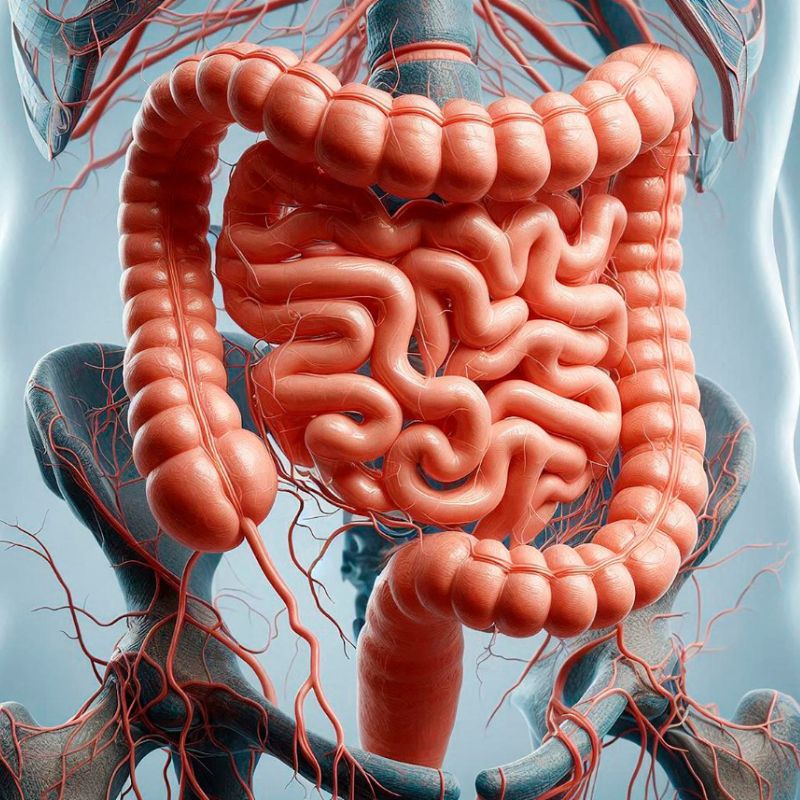
The Role of the Small Intestine in Digestion
The small intestine, measuring about 20 feet in length, connects the stomach to the large intestine. It plays a vital role in digesting food and absorbing essential nutrients. Additionally, it houses a network of lymphoid cells crucial for immune system function, helping to regulate immune responses and fight infections.
Bacteria exist in the entire gastrointestinal tract, but their concentration varies:
The bacterial composition in the small intestine should be different from that in the colon. However, when bacterial overgrowth occurs, it can lead to many kinds of digestive and systemic issues.
Understanding SIBO
SIBO occurs when bacterial populations in the small intestine become excessive or imbalanced. This overgrowth disrupts normal digestion and nutrient absorption, leading to symptoms such as gas, bloating, and diarrhea. It may also contribute to malnutrition and damage the intestinal lining if left unchecked.
Although bacteria are essential for gut health, an overgrowth of harmful or misplaced bacteria can lead to discomfort and systemic health issues. Certain species can ferment carbohydrates, producing excess gas, while others may interfere with fat absorption or vitamin synthesis.
How Does SIBO Affect Our Body?

Bacteria in the small intestine break down carbohydrates, producing gas and short-chain fatty acids (SCFAs). When there is an overgrowth of bacteria, this process intensifies, leading to excessive gas, bloating, cramping, and diarrhoea. Additionally, methanogenic bacteria can contribute to symptoms like brain fog and headaches.
Beyond digestive symptoms, SIBO can interfere with nutrient absorption. Bacteria can consume proteins, vitamin B12, and bile salts—substances essential for fat digestion. This disruption can lead to poor absorption of fats, calcium, and fat-soluble vitamins A, E, and K. While these deficiencies may not be immediately noticeable, they can become apparent in chronic cases, particularly to practitioners experienced in identifying them.
Short- and Long-Term Effects of SIBO
Over time, vitamin and mineral deficiencies can lead to chronic fatigue, weakened bones, and even neurological symptoms and chronic mood disorders. If left untreated, the effects of SIBO can significantly impact overall health and quality of life.

IBS and SIBO: A Common Misdiagnosis
SIBO is often mistaken for irritable bowel syndrome (IBS) because their symptoms overlap. Research suggests that between 4% and 78% of IBS patients actually have SIBO—a broad range due to differences in diagnostic criteria and testing methods (Ghoshal et al., 2017).
With such inconsistencies in diagnosing SIBO, it’s no surprise that many cases go undetected or misdiagnosed for years. The true prevalence of SIBO among healthy individuals is unclear, but studies indicate that anywhere from 1% to 40% of symptom-free individuals may have underlying SIBO. (Ghoshal et al., 2017).
Even when SIBO is specifically tested for, the existing diagnostics are not always accurate. (Rao et al., 2019). I’ve always recommended caution when relying on SIBO test results for this reason. We call it paralysis from analysis.
SIBO Symptoms
The symptoms of SIBO can be difficult to assess and correctly diagnose. This functional gut problem can easily mirror several different gut problems. Depending at what stage your SIBO is, you may experience any of the following symptoms:

Chronic Indigestion, Bloating and Diarrhoea
SIBO is often linked to chronic digestive issues such as bloating, gas, and diarrhea. Research suggests that SIBO plays a significant role in underlying gut disorders (Dukowicz et al., 2007).
In some cases, individuals with SIBO experience unintentional weight loss and struggle to absorb essential nutrients, leading to deficiencies that can impact overall health. Left unchecked, SIBO may contribute to leaky gut syndrome and multiple food intolerances.
Many people assume that SIBO only affects a small percentage of individuals, such as those with structural abnormalities in the upper gastrointestinal (GI) tract or those with conditions that impair GI motility. However, SIBO may be more prevalent than previously thought.
SIBO Symptoms Often Go Undiagnosed
SIBO is believed to be frequently underdiagnosed in clinical settings. Mild cases may present with little to no symptoms, while more severe cases can cause a range of non-specific digestive complaints that often mimic other conditions, such as irritable bowel syndrome (IBS). Just like Candida yeast infections, SIBO remains elusive to many healthcare professionals.
Patients with SIBO commonly seek treatment for various gut-related symptoms, including:
Depending on the severity of symptoms, treatment approaches may involve dietary changes, pharmaceutical interventions, herbal antimicrobials, or targeted nutritional supplements.
SIBO Die-Off Symptoms
During SIBO treatment, particularly with antibiotics or antimicrobials, a phenomenon known as the Herxheimer reaction, or “die-off,” may occur. This reaction results from the rapid killing of bacteria, releasing endotoxins into the system and temporarily exacerbating symptoms. Common die-off symptoms include:
Prompt recognition and treatment of SIBO are essential to prevent these complications and maintain overall health.
SIBO Causes
Your body relies on a complex network of chemical and mechanical processes to maintain a balanced gut microbiome. When one or more of these systems fail, bacterial overgrowth can occur. SIBO develops when the mechanisms that regulate bacteria in the intestines break down, allowing bacteria to migrate to areas where they shouldn’t be.
Reduced Intestinal Motility
SIBO primarily involves bacteria from the large intestine moving into the small intestine. This “retrograde migration” disrupts normal gut function, leading to the symptoms associated with SIBO.
Essentially, bacteria that belong in the colon begin back-flowing into the small intestine, where they shouldn’t be.
One of the key contributing factors to SIBO is reduced intestinal motility—the movement of food through the small intestine. Studies indicate that 90% of SIBO cases are linked to motility disorders in the small intestine (O’Mahony et al., 2010). When food moves too slowly, bacteria have more time to multiply and overgrow.
Bacteria and Gases Involved in SIBO
SIBO is linked to the overgrowth of various bacteria, including:
These bacteria produce gases such as hydrogen, methane, and hydrogen sulfide, which contribute to bloating, discomfort, and digestive disturbances.
In methane-dominant SIBO, the primary methane-producing microorganism is Methanobrevibacter smithii, part of the archaea family—organisms similar to bacteria but distinct in function.
How SIBO Develops
SIBO often starts when food doesn’t move efficiently through the gut, leading to:
We will discuss these gas-producing bacteria in more detail later when we cover SIBO breath testing. But first, let’s explore how food movement through the gut is regulated by the Migrating Motor Complex (MMC) and its role in preventing SIBO.
The Migrating Motor Complex (MMC)

The MMC is a natural muscular contraction pattern in the stomach and small intestine. It acts like an “intestinal broom”, sweeping food and bacteria through the digestive tract. This cleaning process occurs between meals and is interrupted only when you eat.
The MMC plays a crucial role in preventing SIBO by moving food particles from the small intestine to the large intestine. When this function is impaired, the process slows down, allowing bacteria from the large intestine to migrate back into the small intestine (Deloose et al., 2012).
Certain conditions can disrupt the MMC and increase the risk of SIBO, including:
How Your Body Prevents SIBO
Your body has several built-in mechanisms to prevent bacterial overgrowth in the small intestine:
SIBO is typically caused by a combination of factors affecting one or more of these protective mechanisms. Certain risk factors increase the likelihood of developing SIBO, which we will explore in more detail later. For a deeper look at associated conditions and risk factors, see studies: (Dukowicz et al., 2007) (Bures et al., 2010)
8 Common SIBO Causes

SIBO is a complex condition influenced by factors like impaired motility, anatomical abnormalities, enzyme deficiencies, immune dysfunction, medication use, and diet.
Identifying these causes helps in diagnosis and treatment, leading to better symptom management and gut health.
However, evidence regarding SIBO’s causes can be speculative, and healthcare conclusions may not always be fully reliable.
In fact, while research continues to uncover contributing mechanisms, many cases of SIBO still present with unclear origins, suggesting that many factors interplay between our gut bacteria, our host physiology, and our lifestyle factors, which makes personalised SIBO Treatment approaches essential for lasting relief.
Let’s explore the most plausible causes. From my clinical experience, most cases stem from three main causes, which we will discuss shortly, here are the main contributing factors:
Contributing Factors to SIBO
Top 3 Causes of SIBO
Chronic or recurrent SIBO is often a symptom of an underlying problem. Addressing the root cause—not just treating the overgrowth—is key to long-term relief. In most cases, I have found SIBO is caused by:
SIBO is more likely if your gut immune system is compromised. Overgrowth can inflame the intestinal mucosa, worsening gut pain and bloating. In some cases, biopsies reveal flattened villi, thinned mucosa, and increased white blood cells, particularly in older adults with SIBO.
The Connection Between Antibiotics and SIFO
Antibiotic prescriptions often lead to SIFO (Small Intestinal Fungal Overgrowth).
This is why it’s critical to properly identify whether SIBO or SIFO is present before using antibiotics. Treating the wrong type of overgrowth can make gut problems significantly worse

The Role of the Ileocecal Valve (ICV)
What Is the Ileocecal Valve?
The ileocecal valve (ICV) is a crucial one-way valve located between the small and large intestines. Its function is to prevent the contents of the large intestine from refluxing back into the small intestine.
A study found that those who test positive for SIBO often have ileocecal valve dysfunction, allowing bacteria to migrate backward into the small intestine (Miller et al., 2012). This retrograde reflux contributes to the bacterial overgrowth seen in SIBO patients.
Tender Abdominal Spots and the ICV Connection
Patients with chronic gut problems often report tenderness in specific abdominal areas. One common trigger point is located on the right side of the abdomen, near the ileocecal valve region. Symptoms associated with ICV dysfunction include:
In our clinic, we’ve seen many so-called “mystery” cases where patients presented with unexplained pain in this region. In time, these symptoms cleared up once herbal treatments targeted the underlying bacterial, yeast, or parasitic infections affecting the ICV.
Final Thoughts
For years, the medical community dismissed gut dysbiosis as fiction. Today, SIBO is recognised as a legitimate condition with a clear bacterial component. However, the best results come when treatment goes beyond just bacteria and addresses yeast overgrowth as well. By using natural antimicrobial therapies, supporting the gut microbiome, and understanding the role of the ileocecal valve, we can achieve long-term relief for those struggling with SIBO.

What Is A Functional Medicine Doctor?
Functional medicine (or integrative medicine) doctors are medical doctors who use specialised training and techniques to find the root causes of complex chronic illnesses. Some have trained in naturopathic medicine as well. A doctor in functional medicine works holistically, considering the full picture of your physical, mental, emotional, and sometimes even spiritual health. You can find a functional medicine doctor in your area by clicking on this link.
But, if you can’t for some reason work with a functional medicine doctor, a naturopathic doctor, or other health-care professional with SIBO experience, we recommend using your symptoms as a guide, and to follow our diet and treatment recommendations.
Tests For SIBO
The Past-Approach to Gut Issues
For decades, conventional medicine would often dismiss gut-related symptoms with vague diagnosis such as “food allergies”. I recall many patients undergoing scratch (RAST) or blood-based allergy tests, yet results mostly came back normal.
In other cases, doctors assumed patients with persistent digestive symptoms had “parasites” or suffered from recurring “food poisoning”. Stool sample tests were commonly performed yet in most cases they found nothing conclusive. Yet, despite a lack of findings, the standard medical response was to prescribe “pre-cautionary antibiotics”. This was—and often still is—common medical practice, although an increasing amount of GPs are becoming aware of increasing antibiotic resistance.
While antibiotics provided temporary relief, symptoms frequently returned once the course ended. This treatment cycle confirmed what I had long suspected: that gut imbalances often aren’t simply bacterial, but involved yeast overgrowth as well. This was further confirmed when the patient was followed-up with comprehensive stool testing in many cases.
Challenges in Diagnosing SIBO
Even when SIBO is specifically tested for, current diagnostic tools are not always reliable. This is why I often advise caution when interpreting SIBO test results. Relying too heavily on testing without considering clinical symptoms can lead to paralysis from analysis.
Studies have found that the gold standard when it comes to SIBO and SIFO testing is endoscopic small bowel aspiration. This method however is invasive and certainly not without risk to your health (Karunaratne et al 2020).

Comprehensive Stool Testing
The Importance of Stool Testing for SIBO
Comprehensive stool testing serves as a pivotal diagnostic tool in evaluating gastrointestinal (GI) health, offering insights into digestion, absorption, inflammation, and the gut microbiome. According to research, when a stool test is performed properly it has substantial practical diagnostic value in patients with chronic diarrhoea with no known cause (Steffner et al., 2012).
While traditional methods like lactulose breath tests are commonly used to diagnose SIBO), they may not provide a complete picture of our gut health.
Integrating comprehensive stool analysis can uncover additional factors contributing to our gut health symptoms, thereby facilitating more targeted and effective treatment strategies.
Let’s now take a quick look at a few key SIBO markers found in comprehensive stool tests:
Key Markers Assessed in Comprehensive Stool Testing
A thorough stool analysis evaluates several critical markers that reflect the overall status of the GI tract:
The Role of Stool Testing in SIBO Evaluation
While SIBO specifically pertains to bacterial overgrowth in the small intestine, comprehensive stool testing primarily assesses the large intestine’s microbial environment. However, stool tests can reveal imbalances and infections that may influence or mimic SIBO symptoms.
For instance, identifying pathogenic bacteria, yeast overgrowth, or parasitic infections through stool analysis can inform a more holistic treatment approach, addressing issues beyond bacterial overgrowth alone.
Advantages of Comprehensive Stool Analysis
Incorporating comprehensive stool testing into the diagnostic process offers several benefits, but here are the key three advantages of this form of testing, and why it was always been one of our preferred methods in our clinic for many years:
In conclusion, while breath tests remain standard for diagnosing SIBO, comprehensive stool testing offers a broader evaluation of GI health. By identifying additional factors such as inflammation, immune response, and microbial imbalances, stool analysis enhances the understanding of a patient’s digestive health, leading to more comprehensive and effective treatment strategies.
Common SIBO Patterns in Stool Tests
Diagnosing SIBO primarily involves breath tests and, in certain cases, direct cultures from the small intestine. While comprehensive stool analyses are valuable for assessing overall gut health, their direct role in diagnosing SIBO alone is limited.
However, specific patterns observed in stool tests can suggest the presence of SIBO:
A comprehensive diagnostic approach, including clinical evaluation and appropriate testing, is essential for accurate identification and management of SIBO.

SIBO Breath Testing
Small Intestinal Bacterial Overgrowth (SIBO) is commonly diagnosed using breath tests that detect specific gases produced by bacterial fermentation in the gut. The primary gases measured are hydrogen and methane, which are byproducts of carbohydrate fermentation by intestinal microbes.
Testing Procedure
Patients undergoing a SIBO breath test consume a carbohydrate drink, typically glucose or lactulose. After ingestion, breath samples are collected at regular intervals to measure concentrations of hydrogen and methane gases. Elevated levels of these gases within a specific timeframe can indicate bacterial overgrowth in the small intestine.
The SIBO breath test is very narrow and specific in terms of what it offers – it tests for the presence of bacteria based on the types of gas your gut produces, hydrogen or methane. Hydrogen is the predominant gas generally found, and this test is also called the hydrogen breath test (HBT). (Tansel et al., 2023)
Types of Breath Tests
Limitations of Breath Testing
Breath tests, while non-invasive and widely used, have several limitations:
Hydrogen and Methane Producing Bacteria
The gases measured in breath tests are produced by specific microbial populations in the gut:
Caution If Relying Only On Breath Tests For SIBO Diagnosis
A study however has mentioned that regular use of the lactulose breath test in the evaluation of symptoms in patients with suspected functional gastrointestinal disorders “cannot be recommended”. (Simrén et al., 2006) It’s not surprising, because the sensitivity and specificity of the breath tests isn’t the best in detecting SIBO:
To complicate these matters further, studies have found the most used tests, the breath tests (measuring levels of hydrogen and methane gas), have high rates of false negatives. False negative meaning the test results come back as negative, but you may still have a bacterial problem. (Dukowicz et al., 2007)
Take-Away
Breath testing remains a valuable, non-invasive tool for diagnosing SIBO, despite its limitations. Understanding the nuances of test types, potential inaccuracies, and the nature of gas-producing bacteria is essential for accurate diagnosis and effective treatment planning.
For comprehensive information about SIBO treatment and management, including SIBO diet and supplementation, click here: SIBO Treatment
SIBO Study References
Dukowicz AC, Lacy BE, Levine GM. Small intestinal bacterial overgrowth: a comprehensive review. Gastroenterol Hepatol (N Y). 2007. Link
Martins CP, Chaves CHA, Castro MGB, Gomes IC, Passos M. Prevalence of Small Intestine Bacterial Overgrowth in Patients with Gastrointestinal Symptoms. Arq Gastroenterol. 2017. Link
Quigley EM. Small intestinal bacterial overgrowth: what it is and what it is not. Current opinion in gastroenterology. 2014. Link
Ghoshal UC, Shukla R, Ghoshal U. Small Intestinal Bacterial Overgrowth and Irritable Bowel Syndrome: A Bridge between Functional Organic Dichotomy. Gut and liver. 2017. Link
Sachdev AH, Pimentel M. Gastrointestinal bacterial overgrowth: pathogenesis and clinical significance. Therapeutic advances in chronic disease. 2013. Link
Triantafyllou K, Chang C, Pimentel M. Methanogens, methane and gastrointestinal motility. J Neurogastroenterol Motil. 2014. Link
Bures J, Cyrany J, Kohoutova D, et al. Small intestinal bacterial overgrowth syndrome. World JGastroenterol. 2010. Link
Rezaie A, Pimentel M, Rao SS. How to Test and Treat Small Intestinal Bacterial Overgrowth: an Evidence-Based Approach. Curr Gastroenterol Rep. 2016. Link
Lin HC. Small intestinal bacterial overgrowth: a framework for understanding irritable bowel syndrome. JAMA. 2004. Link
Pimentel M, Funsalus R, Rao S, Zhang H. Methanogens in human health and disease. Am J Gastroenterol Suppl. 2012. Link
De Lacy Costello BP, Ledochowski M, Ratcliffe NM. The importance of methane breath testing: a review. J Breath Res. 2013. Link
Kunkel D, Basseri RJ, Makhani MD, Chong K, Chang C, Pimentel M. Methane on breath testing is associated with constipation: a systematic review and meta-analysis. Digestive diseases and sciences. 2011. Link
Rezaie A, Buresi M, Lembo A, et al. Hydrogen and Methane-Based Breath Testing in Gastrointestinal Disorders: The North American Consensus. The American journal of gastroenterology. 2017. Link
Costa MB, Azeredo Jr IL, Marciano RD, Caldeira LM, Bafutto M. Evaluation of small intestine bacterial overgrowth in patients with functional dyspepsia through H2 breath test. Arq Gastroenterol. 2012. Link
Patil AD. Link between hypothyroidism and small intestinal bacterial overgrowth. Indian J Endocrinol Metab. 2014. Link
Pimentel M, Wallace D, Hallegua D, et al. A link between irritable bowel syndrome and fibromyalgia may be related to findings on lactulose breath testing. AnnRheumDis. 2004. Link
Chedid V, Dhalla S, Clarke JO, et al. Herbal therapy is equivalent to rifaximin for the treatment of small intestinal bacterial overgrowth. Global advances in health and medicine : improving healthcare outcomes worldwide. 2014. Link
Vantrappen G, Janssens J, Hellemans J, Ghoos Y. The interdigestive motor complex of normal subjects and patients with bacterial overgrowth of the small intestine. The Journal of clinical investigation. 1977. Link
Pimentel M, Morales W, Rezaie A, et al. Development and validation of a biomarker for diarrhea-predominant irritable bowel syndrome in human subjects. PloS one. 2015. Link
Grace E, Shaw C, Whelan K, Andreyev HJ. Review article: small intestinal bacterial overgrowth–prevalence, clinical features, current and developing diagnostic tests, and treatment. Alimentary pharmacology & therapeutics. 2013. Link
Pimentel M, Chang C, Chua KS, et al. Antibiotic treatment of constipation-predominant irritable bowel syndrome. Digestive diseases and sciences. 2014. Link
Pimentel M, Chatterjee S, Chow EJ, Park S, Kong Y. Neomycin improves constipation-predominant irritable bowel syndrome in a fashion that is dependent on the presence of methane gas: subanalysis of a double-blind controlled study. Digestive diseases and sciences. 2006;51(8):1297-1301. Link
Pimentel M, Lembo A, Chey WD, et al. Rifaximin therapy for patients with irritable bowel syndrome without constipation. The New England journal of medicine. 2011. Link
Pimentel M, Morales W, Lezcano S, Sun-Chuan D, Low K, Yang J. Low-dose nocturnal tegaserod or erythromycin delays symptom recurrence after treatment of irritable bowel syndrome based on presumed bacterial overgrowth. Gastroenterol Hepatol (N Y). 2009. Link
Ploesser J, Weinstock LB, Thomas E. Low dose naltrexone: side effects and efficacy in gastrointestinal disorders. International journal of pharmaceutical compounding. 2010. Link
Cook S. Small Intestinal Bacterial Overgrowth: A clinician’s guide to evaluation and treatment. 2017; http://www.naturalmedicinejournal.com/research-guide-library, 2017. Link
Sandberg-Lewis S, Siebecker A. SIBO: Dysbiosis Has A New Name. Townsend Letter. 2015(February/March). Link
Pimentel M. Review article: potential mechanisms of action of rifaximin in the management of irritable bowel syndrome with diarrhoea. Alimentary pharmacology & therapeutics. 2016. Link
Foxx-Orenstein AE, Camilleri M, Szarka LA, et al. Does co-administration of a non-selective opiate antagonist enhance acceleration of transit by a 5-HT4 agonist in constipationpredominant irritable bowel syndrome? A randomized controlled trial. Neurogastroenterology and motility : the official journal of the European Gastrointestinal Motility Society. 2007. Link
Saller R, Pfister-Hotz G, Iten F, Melzer J, Reichling J. [Iberogast: a modern phytotherapeutic combined herbal drug for the treatment of functional disorders of the gastrointestinal tract (dyspepsia, irritable bowel syndrome)–from phytomedicine to “evidence based phytotherapy.” A systematic review]. Forschende Komplementarmedizin und klassische Naturheilkunde = Research in complementary and natural classical medicine. 2002. Link
Malfertheiner P. STW 5 (Iberogast) Therapy in Gastrointestinal Functional Disorders. Digestive diseases. 2017. Link
Micklefield GH, Redeker Y, Meister V, Jung O, Greving I, May B. Effects of ginger on gastroduodenal motility. International journal of clinical pharmacology and therapeutics. 1999. Link
Kokubo T, Matsui S, Ishiguro M. Meta-analysis of oro-cecal transit time in fasting subjects. Pharmaceutical research. 2013. Link
Shah ED, Basseri RJ, Chong K, Pimentel M. Abnormal breath testing in IBS: a meta-analysis. Digestive diseases and sciences. 2010. Link
Banik GD, De A, Som S, et al. Hydrogen sulphide in exhaled breath: a potential biomarker for small intestinal bacterial overgrowth in IBS. Journal of breath research. 2016. Link
Pimentel M, Chang C, Chua KS, et al. Antibiotic treatment of constipation-predominant irritable bowel syndrome. Digestive diseases and sciences. 2014. Link

Eric Bakker N.D.
Greetings! I am a naturopathic physician from New Zealand. Although I’ve retired from clinical practice since 2019 after 34 years of clinic. I remain passionate about helping people improve their lives. You’ll find I’m active online with a focus on natural health and wellbeing education through my Facebook page, Reddit page and YouTube channel, including this website.





